Subject Code/Name: MED5091 - Advanced clinical practice 1 and
MED5092 - Advanced clinical practice 2Workload: Varies between rotations and sites, but expect to be at your site the same hours as your intern or junior doctor. That generally means 8am - 5+pm for medical rotations, 7am - 5+pm for surgical rotations, and 8-10 hour shift rotations if in the emergency department.
Assessment:- Pre-Intern Appraisals (PIA) (hurdle): there are five of these that need to be filled out by a supervising consultant doctor, one for each rotation (none for the elective rotation) and each worth 18% of Year 5
- Clinical Knowledge Test (CKT): the only exam for the year, is MCQ/EMQ format and is done at the end of the year, not a hurdle to pass but a hurdle to attend (which is unusual), worth 10% of Year 5
- Modules: a variety of paper, online, and in-person module tasks aimed to supplement clinical learning, many of which are hurdles, for each rotation; the sites and supervisors choose how exactly they want these done (more on this later), none of these count towards the final Year 5 score
- Attendance: a very strict expectation of 100% attendance, although technically the lower bound is 80%
Recorded Lectures: Yes.
Past exams available: Yes there is a practice CKT available from the Faculty.
Textbook and Website Recommendation: This is a year where textbooks should be utilised only if you really need to, as most of the learning should be occurring during working hours and not at the desk (unlike Year 4!). Personally, I'd strongly recommend at least having a look at the Australian version of "Marshall & Ruedy's On Call: Principles & Protocols", as it is a relatively succinct text on everything practical than an intern will be doing for patients on the ward (minus the paperwork!). As for other resources, as per my reviews of previous units and years, I'd also recommend utilising UpToDate, eTG, and
http://radiopaedia.org/ as much as possible.
Lecturer(s): Many, depending on the series of lecture
Year & Semester of completion: Semester 1 and 2, 2017
Rating: 5/5
Comments: These units are code for a "pre-internship" year. In my opinion, I found this to be the best year of medicine, but undoubtedly, it comes with many challenges. I'll try to order my comments here in a logical fashion.
Structure of the yearSo Year 5, of which these units account for the vast majority of (so I'll use them synonymously with 'Year 5' for my ease), is divided into 6 rotations, each 6 weeks long, with a week of lectures (and the CKT) at the end of the year. There is a three week gap after the first three rotations, for reasons that will become apparent later in this review, I wouldn't call these a holidays. There is only the weekend in between each of the other rotations.
The six rotations are:
1. Medicine
2. Surgery
3. Emergency
4. Aged care
5. Specialty
6. Elective
Obviously, these rotations are not necessarily in this order. Speaking of which, it's worth touching upon how you get to choose your rotations and what my tips and tricks are. The Faculty sends out an email with your rotation allocations towards the middle of Year 4, this will be a generic email saying that you got your Medicine rotation (for example) at Rotation 5 and so forth. These rotations are not set in stone, and you can swap them. My tip is to NOT have your elective in the first two rotations of the year, and ideally not in the first half of the year. This is because, internships, which I'll touch upon towards the end of my review, need referees and these need to be from Australia (preferably: Victoria) so best to have some Victorian rotations before those intern applications are due.
After this initial allocation you are allowed to preference for individual rotations, which occurs towards the end of Year 4. The exact process has escaped my memory, but I think you get to preference 10 rotations for each allocation, but only a maximum of two rotations from the one site. So for example, you can only preference The Alfred twice for a medical rotation. As with any preference system, the highest one should be the one you want the most. The specialty rotation I'll talk about later, but it's essentially a mix of the more obscure medical specialties, surgical specialties, and other specialties (including the weird and wonderful such as a rotation at the Victorian Institute of Forensic Medicine). The Elective rotation is left for later,and can essentially be done anywhere that offers a 6 week rotation with a single supervisor.
The only caveat with rotations for domestic students to be aware of, is that if you haven't done a rural year in Years 3 or 4, then you have to do a least one 6 week rotation in a rural area. What I'd advise is, choose which of the 5 rotations you would want to do in a rural area, and for preferencing in that rotation, ONLY list rural sites. For the other 4 rotations, list NO rural sites unless you want to do more time rurally. The rule of thumb is: if you preference it rural anywhere in your list, you'll get it, so be aware of this. Personally, I chose to do my Surgical rotation in rural Mildura to escape early wake-ups and Melbourne winter, and I also did my Aged care rotation in Bendigo in the brand new hospital - I loved both rotations and would therefore recommend rural rotations to everyone.
As for what preferences most people got, I think I got four first preferences, and one that was somewhere else on my list. Most people probably aren't so lucky, but generally do get at least one top preference in their final allocation. These final allocations are revealed to you via email in late September.
Before starting each individual rotation, it's worth checking the handover sheet. This is a Google spreadsheet that students are encouraged to fill out once they have completed a rotation, and provides tips and tricks about the rotation. Ideally, every student would fill this out, but in reality it's probably less than 25% per rotation, which is a real shame. Regardless, hopefully you find that some decent soul has filled in something for your upcoming rotation, so you know what you're heading into.
Medical rotationMedical rotations are my love, so I thoroughly enjoyed my rotation. I was fortunate enough to do a rotation at one of the large tertiary networks in an area that I am super interested in, and I tried to make the most of it. Obviously detailing my rotation would be of very limited use to most of the people in the degree, so here is my general advice:
- This is a rotation where you can really hone in on your intern skills. There will be plenty of opportunities to make the intern's life easier by doing procedures on the ward, doing discharge summaries, writing the ward notes, making referrals, etc. Try and do as much of this as possible as you'll inevitably have to do a Gen Med rotation next year where all of this is bread and butter. Should be noted, that anything you do should be run by your intern and should be checked by your intern, especially official hospital documentation. Technically, you should not be writing on drug charts or writing scripts, but definitely try and get some exposure to them.
- Just to reinforce this: for all the above, it's unlikely you'll have an intern who will hand you these opportunities on a platter. You have to seek them out, you have to be keen. I promise you that it will pay dividends for not only your transition into next year, but also how the consultants are registrars will view you. You want to be viewed as a member of the team, not another medical student. This is the key. I tended to stay doing jobs until 7pm some days, and as a result I had an amazing rapport with the team and was always invited to join out-of-hours rounds on interesting cases, Friday evening beers, extra clinics, and so forth. Be keen and helpful, and you'll learn way more.
- With that said... you are still a student. So don't be a slave. You're there to learn, not do all the boring work while your intern deals with the fun stuff. It's a fine balance between pulling your weight and learning. One way to make sure you get enough of the latter is to do what med students do: see patients. Try and be at the admissions (or do them yourself!), report back cases to your registrars when they have time, and ask questions. This is the last time you have to ask questions without feeling too stupid, so make the most of it!
- Do your pre-readings. It should be obvious, but if you're entering a rotation on Lung Transplants, and you haven't got a clue what they're about, you should really smash out some readings on the weekend before. UpToDate is my personal fav for seeking out information in a rush, so that's what I'll recommend. But seriously, you'll look like an idiot if you can't answer the basic questions you may be asked, and you'll also be lost for a good chunk of the rotation which negatively impacts on your learning opportunities.
- Onto something particular: discharge summaries. These are something that I wasn't taught how to approach, and it really took me reading a lot of summaries and doing heaps myself until I developed a format which I found to be reproducible across simple and complex patients in multiple medical and surgical specialties. Here's how I like to go about tackling these pesky beasts:
Mr/Ms <name> is a <age> year-old male/female, from <home situation>, who presented to <hospital> emergency department on <date> with <presenting complaint>, this is in the setting of <anything recent>, and on an active background of <relevant past medical history>.
Presenting
- In dot points, briefly describe the presentation
- Include a dot point of pertinent negative findings (eg. clinically ruling out sepsis, or APO, or an ischaemic limb, etc.)
- In dot points, describe what was done in emergency, including summarising relevant examination (including vitals) and investigations
- Sample line 1: "Although previously well, developed sudden-onset weakness of L) hand and arm while driving at 12.14 pm"
- Sample line 2: "Immediately pulled car on side of road, and called for an ambulance, which arrived at 12.35pm and brought him to hospital"
- Sample line 3: "He reported no infective symptoms (cough/dysuria/neck stiffness/fevers/rigours), no pain, no headache, no loss of consciousness, no visual symptoms, no recent surgery or trauma"
- Sample line 4: "Notably, he had not been taking his aspirin or antihypertensive medications for the last week"
- Sample line 5: "At presentation, he was haemodynamically stable with a regular pulse and manual blood pressure of 150/85 mmHg, he was afebrile and emergency doctors only noted 4/5 weakness in his L) upper limb with an otherwise unremarkable examination"
Admission
- In dot points again, just describing what happened when your team met the patient, I don't always include this section but do if it's a complex case
- Include any new findings on the physical examination (relevant only) and what management took place from your team
- Sample line 1: "On examination, Mr Smith was haemodynamically stable with a regular pulse, and afebrile with a GCS of 15; as noted earlier, he had reduced 4/5 power in his L) upper limb across all movements when compared to the contralateral side, accompanied with brisk reflexes and a subtle increase of tone, notably his cranial nerve and lower limb neurological examinations were unremarkable, as were his chest/heart/abdominal examinations"
- Sample line 2: "Given his presentation suggested an acute stroke, a CT brain was performed which was unremarkable, followed by a CTA whcih demonstrated an occlusion of the R) M2, and a CTP which demonstrated a perfusion mismatch in the R) hemisphere with a large penumbra, features which all suggest an acute ischaemic stroke"
- Sample line 3: "After consultant discussion, it was decided that alteplase be given as per protocol, and this infusion was started at 1.06 pm when Mr Smith's blood pressure was 140/80 mmHg, he tolerated the infusion well in the emergency department"
- Last line of this section should be "Admitted under <home team> on <date> after discussion with consultant Dr <name>"
Progress
# Issue 1
- Dot points again, just detail what happened for each individual issue, give the issue the best medical name possible (eg. Hypertension is better than "Increased blood pressure")
- Include clinical improvements, deteriorations (eg. MET calls, code blues), trends in investigations, impressions by allied health staff
- Sample line 1: "He/She progressed well on the ward, tolerating the increased dose of frusemide well, with a clear chest noted by 29/11 and a clear CXR noted by 30/11."
- Sample line 2: "Allied health input was sought, and Ms Smith began hand exercises and rehabilitation with the physiotherapists on the ward, her strength in that R) hand improved to 4+/5, which was close to her reported baseline"
# Issue 2
- Same deal, for as many issues as is required
Discharge
- Brief, stating discharge rationale, destination, and plan for patient and the GP
- Sample line 1: "With good progress from Neurology and Allied Health points of view, Mr Smith was discharged home"
- Sample line 2: "Several changes were made to Mr Smith's medication regimen, including the addition of <medications and doses and frequency>, and these were explained to Mr Smith by our pharmacist on the ward"
- Sample line 3: "Mr Smith is to follow-up in our Stroke clinic in 4 weeks time and is to have a brain MRI beforehand, and is advised to follow-up with his GP in one week to reassess his hypertension"
There are often other sections of the discharge summary form, depending on where you are, but at some point (after all the above if there isn't a specific area for this), you should mention:
- All the medications to take upon discharge: name, dose, frequency and why
- Which medications have been ceased and why
- Past medical history - often this can be copied from a previous summary, but obviously read and update this
- Actual results, I personally liked to attach scan results verbatim, the latest bloods, and any other important investigations (eg. nerve conduction tests, EEGs, HbA1c, etc.)
- Smoking and alcohol status
- Relevant social history
- Your name and role, your registrars' and consultants' names and roles
- A final note about the modules for this rotation: it depends on your team. There are NO hurdle modules for medicine, so do whatever your supervising consultant wants you to do. Keep in mind, that if you do need to do some, they're quite time-intensive so don't leave them until the last day because you'll struggle.
Surgical rotationAn area of medicine I appreciate, but not one I enjoy at all. As aforementioned, I did this rotation in a rural setting, and for someone who doesn't love surgery, I think this was ideal for seeing a good variety of things, and to nail some of the basics. Obviously again, detailing my rotation would be of very limited use to most of the people in the degree, so here is my general advice:
- Again, be keen. This is how you get things done, this is how you learn heaps, this is how you score well on your PIA. In surgery, the best way to show you're keen is to make it into theatre. I probably scrubbed up more in this single rotation than in the entirety of my previous medical schooling! On some days I was in theatre helping out with cases until 9.30pm. Even though I'm not a fan of surgery, this was enjoyable and the surgeon could see that I wanted to learn and as a result, got me involved in whatever she was doing. Because I was so keen, I even got to present at the Grand Round with my ward partner which was a great experience. Awesome.
- Again, this is another perfect rotation to nail down those basic intern skills. Get the procedures in, get the ward notes in, get the discharge sumamries done. I was a bit of a discharge summary fiend in this rotation and probably did around 35. Amazing practice for the next year, I feel really comfortable about efficiently doing them now. Oh, and the intern was super thankful because it was a very busy unit.
- I feel like I'm repeating myself here a bit, but do your pre-readings! The first and foremost in surgery is the anatomy. Look at the list of cases the day before they happen and read up on the procedures that will happen, and read up about the relevant anatomy. Don't be that guy that walks into a lap cholecystectomy and doesn't know what Calot's triangle is... Never be that guy. As with my advice in third year, worst that happens is that you don't know and say "Honestly not too sure, how about I read up on it tonight and briefly tell you the answer tomorrow?". A response like that shows initiative and shows a certain desire to improve and learn.
- A final note about the modules for this rotation: they are all hurdles. This means you HAVE to do ALL of them. They are actually quite time-intensive so don't leave them until the last day because you'll struggle.
Emergency rotation- This rotation is the traditional favourite for medical students. Wasn't my favourite, but that's not because it wasn't amazing (it was!), but just because I felt I had so many great rotations that this one didn't manage to top the list. Students love it because you get freedom to actually practice medicine. Generally, shifts are 8-10 hours long, and 3-4 shifts per week, although if you're keen you can do more shifts as long as it doesn't impede on the learning of others.
- Just a note on the format of EDs, each is different (of course), but generally there are different streams, some more acute than others. Get a good taste of each stream as you do your rotation. Personally, I found the acute streams (but not the super acute/trauma) streams really good for learning as I did a lot there.
- That leads me what you do in the ED. I think what you do exactly depends on where you are. If you're at a fancy big tertiary centre, you'll be doing a bit of ED work and a bit of shadowing work. If you're at a smaller centre, you'll be doing way more ED work.
- The other factor that alters how much freedom you have is what your consultant thinks of you. If your consultant rates you highly, you'll have free reign, if they think you're a bit of a battler, you'll be reeled in a bit. I think that judgement is made over the first few shifts, and is generally a fair assessment. Nothing wrong with more supervision so don't take it the wrong way.
- Personally, I was fortunate to be treated like a resident. I would pick up my own patients (letting the in-charge consultant know of course!), clerk them, examine them, and report back to the in-charge consultant with my management plan. This is not dissimilar to what any junior doctor would be doing, and is a really good chance to learn. Again, a great chance to refine your procedural, history, and examination skills; you should be busy doing something all the time in the shift!
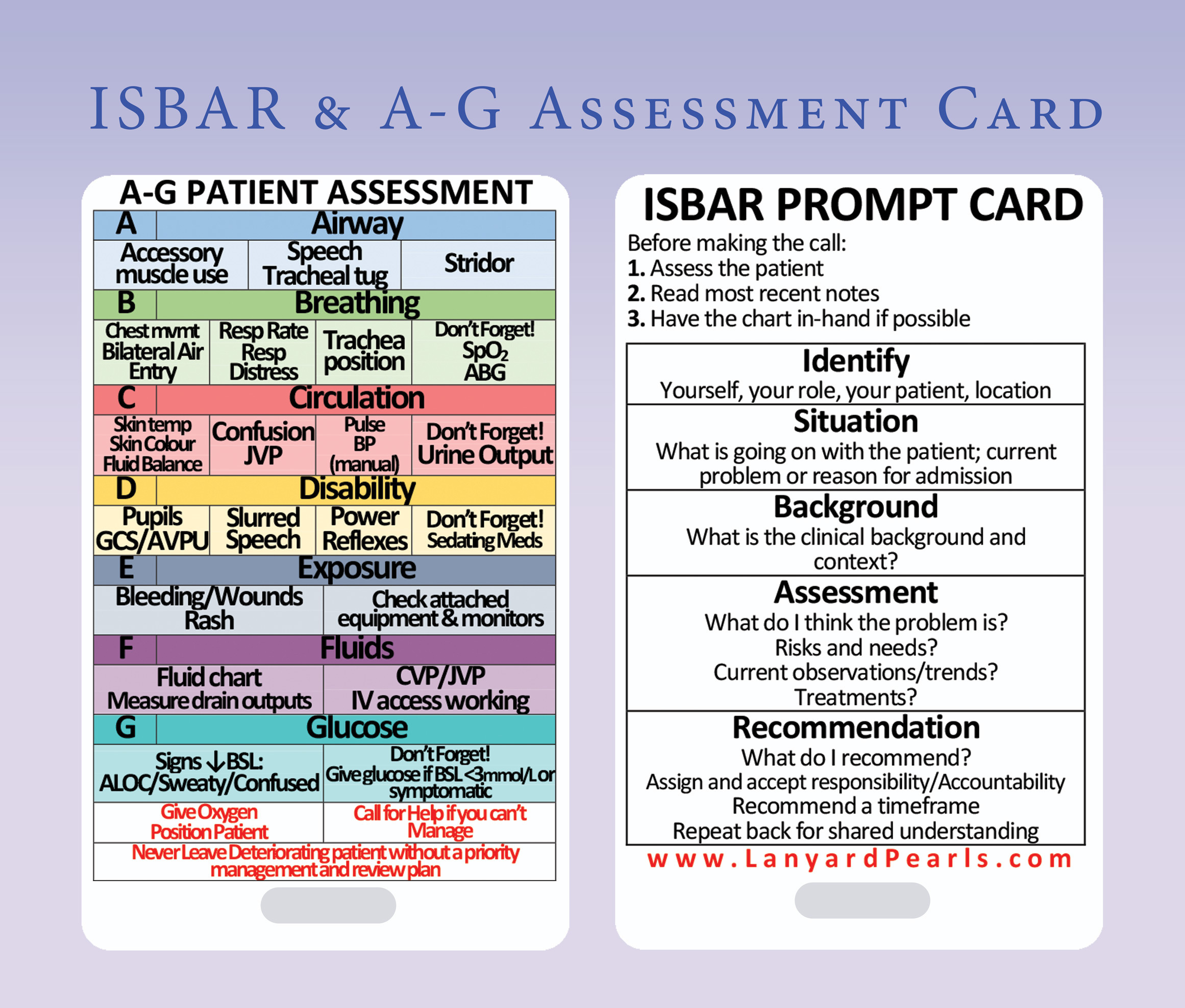
- As part of your management plan, you may be required to make referrals or ask specialties for advice. I always volunteered to take this job on, because again, it's great learning and experience. There are ways to handover patients, and ways to handover patients, and we're all pretty pathetic at it when we start off (and perhaps I'm still not great!), but what is essential is that you're prepared and have a format. By prepared, I mean have the patients' details and results in front of you and ready to go, know the case, know what you're asking of the person you're talking to, and realise that their time is valuable. By having a format, I mean something like ISBAR. This is great, and I use it often. However, there are variations, and I'll attach a couple of useful slides below to guide you. Practice makes better when it comes to referrals.

- A final note about the modules for this rotation: they are all hurdles. This means you HAVE to do ALL of them. They are actually quite time-intensive so don't leave them until the last day because you'll struggle (see the pattern yet?).
Aged care rotation- Not going to post much advice for this rotation, because it's essentially just a medical rotation with elderly patients. The same rules apply.
- Where this rotation differs is in some of the extra-hospital placements you have to do. This includes a visit to the Alzheimer's Association, attending a VCAT hearing, an Aged Care Services visit, and a visit to an aged care facility. Each of these has a worksheet to complete, and these are all hurdle tasks.
- In addition to these extra-hospital visits, there is also the "Interprofessional Learning Day" which is a full day where you learn some aged care bread and butter alongside nursing students. I actually found this day to be pretty useful, despite the doubts I had about it beforehand. So keep an open mind and be kind to each other. It's a good initiative from the Faculty and also a hurdle task.
- The modules in this rotation are also all hurdles, and require you to seek out patients and present them to a consultant. So naturally, these need to be planned in advance with your supervisor. Worth getting on top of finding cases early, especially if your rotation is at a specialised service.
Specialty rotation- Specialty rotations can be anything from a medical rotation, to a surgical rotation, to psychiatry, to paediatrics, to radiology, to pathology, to the weird and wonderful like the Victorian Institute of Forensic Medicine. Hopefully you're allocated something that you enjoy.

- No specific advice for this, it all comes together with the advice from the previous rotations.
- The modules for this rotation are odd. Regardless of whatever you do, there is a Women's Health quiz that needs to be passed on Moodle; this isn't an easy quiz and there are pre-recorded lectures you should watch before attempting it. There is also an essay on HIV that needs to be written, this can be an opinionated piece or a creative piece (I chose the latter) and is quite an interesting task if truth be told. Both of those tasks are hurdle requirements. There are other non-hurdle modules that you may be asked to do by your supervising consultant, such as dermatology and so forth. Fortunately, I wasn't required to do any of that.
Elective rotation- Hopefully you've left this towards the back half of the year as per my earlier advice! Why will become apparent in the next section.
- This is a rotation with a lot of freedom, you can go virtually anywhere in the world that offers a 6 week rotation with a single supervisor. If you're not keen to travel, that's more than fine, Monash offers many rotations that students can choose from in order to do their elective in Victoria.
- If you're going overseas, plan it early. Many places, especially the UK, have very early deadlines for applications, often before the year has even started. So get organised early to avoid disappointment.
- If you're choosing a Monash elective, a list of available rotations will be emailed to you and you then choose which one you want. Time is key here as these are offered on a first-come-first-serve basis.
- No modules for this rotation and no PIA for this rotation, but there is an "Elective Report" that needs to be submitted as a hurdle. This can literally be be on anything as long as it's relevant to your experience. Furthermore, instead of the PIA, there is a "Supervisor's Report", which needs to also be submitted before a deadline date.
Back-to-base and the CKT- 'Back-to-base' describes the phenomenon of coming back to Monash Clayton for some lectures that contain useful knowledge for any junior doctor. In general, I found them to be worthwhile and high-yield.
- These happen on the last Friday of every rotation for a half-day. If you can't make them, they're recorded, however the expectation is that you will be there.
- These lectures also occur at the end of the year for one week, known as the 'Back-to-base week'. This is a jam-packed week, with lectures from a variety of senior and junior doctors on core topics. Excellent revision, lunch included, and note that the roll was taken one day so be sure to turn up!
- During the back-to-base week, there is the CKT. This is really just like the Year 3 exam, but includes more pre-intern knowledge. It's a hurdle to attend, but not to pass (which is strange!). I didn't do any particular study for it, and I think I did fine. Wouldn't lose sleep over it.
That three week gap and internship applications- I've left this to last because technically this isn't part of the units, but it's part of the year, and is arguably the most important part of the year.
- Three weeks off between semesters sounds like a great time to jet of to Europe to discover yourself, right? Wrong.
- This three weeks isn't for holidays, it is when intern interviews occur.
- Now let me back-track a little to explain how this process works. The whole process is mediated by an organisation called the Postgraduate Medical Council of Victoria (PMCV). Consider this the VTAC of medicine. PMCV provides a medium where you can upload your CV and order up to 15 hospitals in a list of preferences. But this is not all you have to do, as each hospital network ALSO requires you to apply to them as well. So it's like VTAC and if you had to apply to each uni as well. It's annoying, I know, but it's what it is.
PMCV- So firstly, what does PMCV require. They need: a standardised CV, your InternZ score, your two referees, and your list of preferences.
- 'Standardised CV' refers to a CV that follows a template created by PMCV. It has fixed sections that need to be filled in and no part of it can be deleted. It can become pretty long (mine was 7 pages I think) if you fill it in correctly. My advice: fill this in at the start of the year, well before any of the internship applications actually open. Refine it as the year progresses. One tip I have is to add subsections to each of their templated tables, for example under the "Leadership roles and extracurricular achievements" section I divided that into the four sections of Leadership, Professional development, Professional memberships, and Extra-curricular; which I felt helped a reader to understand everything that I had done. You can do this, but do not delete anything. The CV also requires a photo (god knows why...), so get this sorted too, it should look professional.
- The 'InternZ score' is hopefully something you're already familiar with. In short, it's calculated using your MED2000 and MED4000 marks such that you're fit along a normal distribution curve that has a median of 3.5. Hopefully, for your sake, you're above 3.5! You get your score towards Rotation 3 time, which is when all the applications start to open up for each hospital.
- The two referees are a source of much stress. PMCV recommends that these be consultants (and indeed some health services will not accept them if they are 'just' Fellows or Registrars!) who have supervised you CLINICALLY in the last 18 months. So basically, from the start of Year 4 until applications are due. Most people get their referees from Year 5, and from Rotations 1-3. This is why I strongly suggest having your exotic elective AFTER these rotations, so you can maximise your chances of having great referees. How to choose a referee is tricky, but generally your consultant supervisor is the best bet. My approach was to ask them towards the end of the rotation if they'd be willing to be your referee (they invariably say 'yes' if you did well on the rotation), and ask for their contact details and ask if they don't mind you sending them a reminder email closer to when applications are due (again, they say 'yes'). I'd then email them a couple of weeks after the rotation is over to thank them profusely and to also attach a mock-PMCV referee template. This template is essentially the assessment that they'll fill out about you once you nominate them as your referee in the PMCV system. The assessment has boxes to tick but also has a comments section, strongly recommend them to write in the comments as health services love the comments. Sending them this early allows them to know what to expect, indeed some keen beans actually printed out the mock template and asked prospective supervisors to fill it out in front of them to see how well they'd give them. Personally, that latter approach is too far, but the email is a nice courtesy. Following this, email them again just before you officially nominate them in the PMCV system, telling them that they'll receive an email from PMCV shortly with a link to a similar form, if they could fill it out promptly AND fill in the comments that would be much appreciated (or something along those lines!). Once they've completed the official form from the PMCV link, you will be notified via email. You do not get to see what scores or comments they gave you, and that's probably for the best. You cannot un-nominate a referee, so choose wisely! To repeat, you need two such referees.
- Finally, the list of preferences. This is straightforward. Essentially just list up to 15 health networks (I did 12) that you'd like to work in. No tricks here, preference the one you want most as #1, the next at #2, and so forth. Victoria has a merit-based system so there's no way to give yourself an advantage of getting a job anywhere through your preferences. The individual hospitals do NOT know where you have preferenced them, and they don't ask either. I wouldn't volunteer the information to them as well.
Health services- Ok that's the PMCV side of it. Now let's talk about the hospital side of it. Each hospital network will have their own online application. You must submit an application for each hospital you preference in PMCV (otherwise... why bother?). The applications vary considerably; some require cover letters, some require you to answer questions, some have extensive forms, etc. You need to actually take some time with each application, and especially take time with the cover letter. Ensure your cover letters are addressed to the right people from each hospital, and ensure that they actually address what the hospital is looking for in an intern. What they're looking for is generally obvious - look at the position descriptions and look at the values of the health service. This all takes a LOT of time, so get onto it when it opens. Worth noting that once you have submitted an application to a health service, you can edit and change it until the deadline, so don't worry too much about getting it perfect the first time, just make sure it's perfect by the deadline.
- One thing to note for the hospitals is that they each run an information session and/or have a stall at the AMA Careers Expo. Worth going to these if you can, you'll have a chance to talk to current staff (senior and junior), learn about the health service, and get tips about applications from them. Some of these require booking in advance (and do sell out!), so be on top of things.
- This whole application process take a LOT of time, and is quite stressful. The best tips I have is to be organised, understand the process, and do things earlier rather than later. When you think you're done with an application, double-check it, and then triple-check it, and then finally check that you've actually submitted it (hint: you'll get an email saying you have).
- Once all of this is due, which is usually towards the end of Rotation 3, you have a peaceful few weeks until interviews are offered. Those few weeks are not a fun time.
Interviews- Onto the interviews. Not all hospitals have them, those that do all do them differently, and they each have mysterious selection criteria. Here are a few hospitals that do them (with style of interview in brackets): Alfred Health (panel interview with HR and consultant doctor, followed by SJT), Austin Health (MMI-style interview with two one-on-one stations, one with a consultant doctor and one with HR), Melbourne Health (group interview), St Vincents Health (panel interview with HR and consultant doctor), Monash Health (video interview, 1 min per question with 2 mins reading). These are generally announced in the first week of the three week break, and depending on the health service, you may get to allocate an interview time slot or it may be auto-allocated. For the interviews, dress formally (more formal than med school interviews in any case), know the health service, know why you want to work there, and have an armamentarium of personal anecdotes that you can slide into answers (eg. about leadership, teamwork, working with difficult staff/patients, etc.).
- Job offers come out towards the end of July, and the wait is generally an unpleasant one!
Overall impressionWhat a year it is. What a fantastic year. You really do feel like you're practicing medicine and making a difference. Yes there are the stresses associated with intern applications and interviews, but I really do think I learnt a great deal from that experience. I think I was fortunate to have a stellar year in terms of rotations, not a rotation I didn't love (even Surgery!), so no complaints from me. That was coupled with me getting decent grades throughout the year, getting the internship spot I wanted at a competitive health service, and even winning an award at graduation. What a damn good year to be part of. It's been an absolute privelege to end my time at Monash Uni on such a high note. Hopefully you have a similarly amazing year too
Feel free to ask me any questions!
